Seizures case
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE DISCUSSION:
20yrs male ,butcher by occupation studied till class 7th.In2011 he had right focal seizures of 1episode and was admitted to the hospital for 1week and used antiepileptic medication for about 2years.In 2014 he had his 2nd episode of rt focal seizures. ?NCC on MRI and was on albendazole and steroids used antiepileptic drugs for 1year and also used herbal medications.

In 2018 he had acute onset of SOB, abdominal tightness and constipation he was admitted in lb nagar kamineni xary was done showing peural effusion and he was diagnosed with TB for which he was prescribed ATT for 6months and stopped the medication on his own without any follow up.





Then on 09-08-2020 @12am patient noticed spasm of right upper limb for 5min and then woke up,then noticed involuntary movements of right upper limb and then to all the limbs.
Uprolling of eyes and head posturing along with tounge bite was present. Post Icteal confusion was present for half n hr.patient had such similar 6episodes-right focal with secondary generalisation.
Patient when presented to casualty was conscious and well oriented.Then he developed involuntary movements of right upper limb which progressed to generalised tonic clonic seizures with uprolling of eyes,head posturing towards left and drooling of saliva.episode lasted for 5min and pt was unresponsive, regained consciousness after 5min with postictal confusion for about half n hr headache present.
No history of neckpain,fever,trauma,neckstifness and weakness.History of rawmeat consumption and pork consumption present.Not a known case of diabetes hypertension and asthma no family history of seizures present.
Ictal cry, bowel and bladder incontinence,aura were absent.
On examination:
Patient is conscious, coherent , co operative
oriented to time , place and person,
moderately built and nourished
VITALS:
Patient was afebrile with
Bp-110/80mmhg
Pulse-86 bpm
RR-22cpm
Spo2-97% at room air
No pallor, icterus,cyanosis, clubbing, koilonychia, lymphadenopathy and pedal edema
CNS: Higher mental functions-normal
Cranial nerves- intact
motor system-intact
Sensory system- intact
No cerebellar signs or any signs of meningeal irritation
GCS-15/15
CVS: s1 s2 heard, no murmurs
RS:BAE present, normal vesicular breath sounds were heard, no added sounds.Traches central in position
ABDOMEN-
Scaphoid in shape,no tenderness and no palpable mass present.Hernial orifices are free.Liver and spleen are not palpable.Bowel sounds are present.
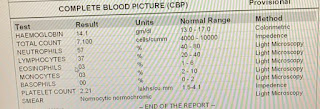
INVESTIGATIONS:









DIAGNOSIS:
EPILEPSY SECONDARY TO LEFT FRONTAL CALCIFIED GRANULOMA ?NCC ?TUBERCULOMA
RIGHT FOCAL SEIZURES WITH SECONDARY GENERALISATION
TREATMENT:
Inj.LEVIPILL 500mg/iv/bd
Inj.MANNITOL100ml/iv/bd
Tab.ALBENDAZOLE 400mg/po/bd
Inj.LORAZEPAM 2mg/iv/sos
Bp charting4th hrly
Spo2and Pr monitoring.
Good share! It helps to know about the patients health data regarding seizures treatment.
ReplyDeleteCheck this too for your information 4 and a half hour window to save a life